Ethnography of traditional healers and their indigenous medicinal plants in southern Philippines: Implications for conservation and sustainable use
Bhegie May G. Buaya,d, Catherine Hazel M. Aguilarb, Maria Celeste N. Banaticla-Hilarioc, Chenny Rose M. Rodriguezd and Florence L. Zapicod,*
a Department of Biology, Institute of Mathematics, Arts, and Sciences, Davao del Sur State College, Digos City, The Philippines
b Global Crop Diversity Trust, Platz der Vereinten Nationen, 7 53113 Bonn, Germany
c Plant Biology Division, Institute of Biological Sciences, University of the Philippines-Los Banos, College, Laguna, The Philippines
d Department of Biology, College of Natural Sciences and Mathematics, Mindanao State University - General Santos, The Philippines
* Corresponding author: Florence L. Zapico (florence.zapico@gmail.com)
Abstract: This paper investigates Indigenous medicinal plants, the threats they face and the healing knowledge and profiles of traditional healers in the Sarangani uplands, Southern Philippines. During field and community floral inventories, 39 medicinal plant species were documented, belonging to 18 orders, 20 families, and 31 genera. While this study unveiled diverse utilization of medicinal plants, interviewed healers unfortunately revealed local losses which they attributed to (1) climate change, (2) overharvesting, (3) forest denudation, and (4) the shift to over-the-counter medicines. Additionally, the gradual erosion of healing knowledge was ascribed to (1) Christianization suppressing traditional healing practice, (2) local losses of medicinal plants, (3) shift in culture and lifestyle brought by increasing market integration, (4) reluctance of tribal healers to share healing knowledge, (5) devaluation of Indigenous knowledge by the younger generation, (6) advanced ages of knowledge keepers, and (7) the oral nature of mentoring. Moreover, this paper reports that conservation was accomplished mainly through continuous utilization/cultivation and the judicious collection of medicinal plants. These efforts are, however, grossly insufficient and without complementary in situ and ex situ conservation initiatives, these invaluable genetic treasures will face local extinction. In addition to Sarangani’s medicinal plant losses, the valuable cache of associated traditional knowledge will likewise be lost, resulting in a culturally impoverished and less resilient community. Finally, to foster inclusivity, promote knowledge pluralism, and aid in the preservation of traditional healing knowledge, the involvement of healers in the crafting of a comprehensive healthcare strategy for Southern Philippines is recommended.
Keywords: Traditional healers, Indigenous medicinal plants, conservation, utilization, Sarangani Province
Introduction
In biodiversity-rich, low to middle-income countries like the Philippines, traditional healing knowledge and medicines remain the primary refuge of ethnic peoples for their healing and therapeutic needs. In rural communities, medicinal plants are abundant, freely available and reputed to be efficacious based on millennia of traditional use (Mahmoud and Gairola, 2013; Bankole et al, 2015; Barata et al, 2016). Indigenous groups have been utilizing Indigenous medicinal plants (IMPs) since time immemorial, leading to a wealth of accumulated traditional healing knowledge (THK). Even up to this time, developed and developing countries alike rely on IMPs as direct sources of medicine or as raw materials for the processing of therapeutic drugs (Miano et al, 2011; Ambasta et al, 2016), thereby resulting in an increasing demand for these priceless natural resources.
Studies from Nepal (Aryal et al, 2016) and Nigeria (Stoffersen et al, 2011; Borokini et al, 2013) report on age-old THK and utilization of IMPs by local communities as well as their economic potentials (Batugal et al, 2004). Known as ethnomedicine, this field of anthropology deals with medicinal plants and the wealth of healing knowledge of traditional healers (Cotton, 1996; Cheikhyoussef et al, 2011). THK is, therefore, an indispensable source of socioculturally coherent information about IMPs, their Indigenous uses, and their natural habitats. Nonetheless, THK is vulnerable to sociocultural and ecological transformations that define traditional communities in contemporary times.
Considered as one of the 18 mega-biodiverse countries in the world, the Philippines ranks fifth in terms of plant species richness (CBD, 2025). Recently, Meniza et al (2024) documented 1,500 species of medicinal plants in the Philippines, with over one-third (or 530 species) found in Mindanao. Recent studies (Dapar et al, 2020; Paraguison et al, 2020; Alinsug et al, 2022; Cabugatan et al, 2022; Ilagan et al, 2022) revealed the prevalent use of medicinal plants in rural Mindanao communities. However, these priceless genetic resources and associated Indigenous knowledge are threatened by emerging social-ecological realities in these areas. Among the identified major pressures to medicinal plant species in the Philippines are agricultural expansion, deforestation, mining, environmental degradation, unregulated resource extraction and climate change (Mendoza et al, 2016; Cordero et al, 2022; Agduma et al, 2023; Belgica et al, 2024). Moreover, Alinsug et al (2022), Dapar et al (2020), Fiscal (2017), and Ong and Kim (2014) reported about the propensity of the younger generation to embrace modernization, resulting in knowledge erosion. Other identified causes of knowledge erosion are acculturation, outmigration and increasing access to over-the-counter medicine (Dapar et al, 2020; Cordero et al, 2022).
At the national level, the Philippine government has been promoting the shift to IMPs, given the exorbitant prices of modern medicines. After thorough evaluation, the Department of Health (DOH) endorsed ten medicinal plants, viz. Senna alata (L.) Roxb., Momordica charantia L., Allium sativum L., Psidium guajava L., Vitex negundo L., Combretum indicum (L.) De Filipps, Blumea balsamifera (L.) DC., Ehretia microphylla Lam., Peperomia pellucida (L.) Kunth and Clinopodium douglasii (Benth.) Kuntze for widescale use (Dapar et al, 2020). Another initiative of DOH was the promotion of herbal medicine gardens in rural communities and the integration of traditional healing into mainstream healthcare (Maramba-Lazarte, 2020). Unfortunately, there is a paucity of information about traditional healthcare practitioners, especially those residing in far-flung areas.
Sarangani Province in Southern Mindanao is home to Lumad (tribes of non-Muslim ethnicity) groups such as B’laans, Tagakaulos, and T’bolis. These groups inhabit remote and inaccessible upland areas and consequently receive no (or very little) basic social services from the local government. Moreover, the lack of government presence in these areas and an official census of the tribal population have resulted in a dearth of information about their exact numbers. These Lumads are, therefore, the most disadvantaged sector of Philippine society, whose dependence on local resources was highlighted when the COVID-19 pandemic isolated their remote communities. This study was thus designed to (1) profile traditional healers, (2), document Sarangani medicinal plants and how they are used in healing rituals, (3) investigate threats to Sarangani medicinal plants, (4) carry out initiatives for evidence-based ex situ and in situ conservation of Sarangani medicinal plants and (5) recommend for the inclusion of traditional healers in the crafting of a comprehensive health strategy. It is envisioned that meticulous documentation of IMP utilization and conservation status will contribute significantly to the preservation of Sarangani traditional healing knowledge for future generations.
Materials and methods
Study locations
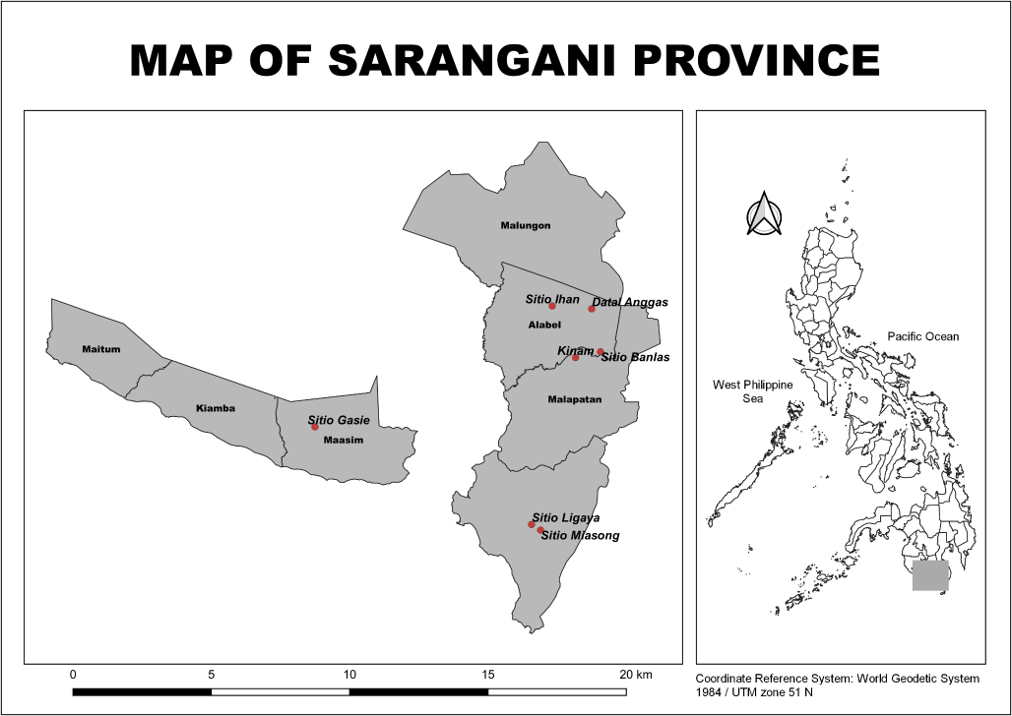
Figure 1 shows a location map of Sarangani Province with all study sites indicated. This study was conducted in seven upland villages (Sitios) in four towns (viz. Kinam and Banlas in Malapatan, Datal Anggas and Ihan in Alabel, Miasong and Ligaya in Glan and Gasie in Maasim) in Sarangani Province. In Malapatan and Glan, B’laans are the predominant tribal group. T’bolis inhabit Maasim while B’laans and Tagakaulos reside in the upland villages of Alabel. The study sites and their geophysical coordinates are shown in Table 1.
Preliminary preparations and ethical considerations
Letters seeking permission for the study were sent to the provincial governor, the mayors, heads of agriculture offices, and barangay (village) captains before field visits. Subsequently, both oral and written consents were secured from healers before the study commenced. Elderly healers who were illiterate appended their thumbprints to the consent form. The participants were informed about the study, its objectives and the information to be solicited from them. They were assured that their identities would be maintained with the utmost confidentiality. Additionally, they were apprised of their right to decline to respond to inquiries or to terminate the key informant interview (KII) at any moment for any personal reason.
Research design, respondent selection, inclusion and exclusion criteria
This study is a qualitative research that employed ethnographic methods, such as direct participant observation, interviews with key informants and a semi-structured questionnaire to chronicle the traditional knowledge of local healers based on their lived experiences. Purposive sampling based on information from sitio officials was utilized to identify potential study respondents. Subsequently, the researchers scoured the remote upland areas of Alabel, Glan, Malapatan and Maasim to locate identified healers. While the municipalities of Maitum, Malungon and Kiamba were initially considered for inclusion in the study, several factors rendered this difficult, if not outright impossible. In Maitum, traditional healers visited by the team declined requests for an interview, believing that divulging secret information would diminish their healing powers. As for the municipalities of Malungon and Kiamba, locals reported shifting to modern medicines and that no more healers were found in the sitios. Moreover, the remoteness and isolation of some villages and safety concerns prevented the researchers from penetrating these far-flung areas.
Table 1. Study sites, their geophysical coordinates and dominant ethnic group/s. IP, Indigenous People; masl, metres above sea level.
|
Sitio |
Municipality |
GPS Coordinates |
Altitude (masl) |
Dominant IP Group |
|
Datal Anggas |
Alabel |
N 06°11.995’ E 125°27.158’ |
900 |
B’laan, Tagakaulo |
|
Sitio Ihan |
Alabel |
N 06°12’21.7” E 125°22’21.7” |
905 |
B’laan, Tagakaulo |
|
Sitio Ligaya |
Glan |
N 05°46’17.5” E 125°19’50.5” |
426 |
B’laan |
|
Sitio Miasong |
Glan |
N 05°45.638’ E 125°20.954’ |
428 |
B’laan |
|
Sitio Banlas |
Malapatan |
N 06°06.508’ E 125°28.065’ |
342 |
B’laan |
|
Kinam |
Malapatan |
N 06°06.125’ E 125°25.0158’ |
406 |
B’laan |
|
Sitio Gasie |
Maasim |
N 05°57.495’ E 124°54.083’ |
1,016 |
T’boli |
The inclusion criteria encompassed traditional healers of any gender, aged 25 years or older, who utilized IMPs for healing and provided explicit consent to participate in the study. A prospective study participant had to be a recognized traditional healer within the community. Conversely, individuals who shifted to modern medicine and those who declined invitations for participation were excluded from the study.
Data collection methodologies and analyses
Ethnobotanical assessment
The semi-structured questionnaire used consisted of open-ended questions, which enabled respondents to articulate comprehensive views regarding traditional healing knowledge in their own words. This questionnaire contained four main sections: (1) demographic profiles of healers and knowledge acquisition, (2) medicinal plants and their modes of utilization, (3) medicinal plant sources, processing and storage, and (4) threats to medicinal plants and conservation awareness. After pre-testing, the validated questionnaire (see Supplemental Material 1) was used as the main data-gathering tool during face-to-face interviews. The questionnaire, written in English, was administered using the predominant dialect of Sarangani (Cebuano) or the tribal dialect through a local intermediary for respondents who could only converse in their native language.
To validate the results of the questionnaire and delve deeper into the healing knowledge of the Sarangani ethnic groups, key informant interviews were carried out. As a qualitative in-depth interview method, a key informant interview is flexible and extracts knowledge from key respondents who have particularly informed perspectives and first-hand knowledge about the topic at hand. Being a descriptive study, answers to the questionnaire and key informant interviews were analyzed thematically, classified a posteriori, and discussed narratively to minimize bias in the conclusions. Subsequently, relevant information was presented in tables for easier reference and interpretation.
Inventory, collection, identification and conservation of Indigenous medicinal plants
Field observation and community walks were conducted to triangulate information and corroborate data from the questionnaires and key informant interviews, thereby lending credence to the results. With the assistance of the healers, medicinal plants were identified and gathered (with consent) from backyards, home gardens, roadsides and adjacent woodlands. Two distinct collection methods were utilized, contingent on the biological characteristics of the plants. For sexually reproducing plants, viable seeds were collected and placed in labelled coin envelopes. On the other hand, vegetatively propagated herbs and seedlings were immediately planted in black polypropylene seedling bags filled with garden soil. Both coin envelopes and seedling bags were labelled with passport information such as the plant’s local name, collection date and site, the name of the household head (if collected in home gardens), and its geophysical coordinates. During community walks, the healers initially recognized medicinal plants by their ethnic names, which were subsequently verified through appropriate references. Collected medicinal plants were classified according to their growth habits and their habitats, among other information. Taxonomic identification was done up to the species level whenever possible using suitable references and consultation with a botanist. No scientific identification was conducted for some IMPs growing deep in the forests, and the researchers relied solely on the healers’ memory and knowledge. Subsequently, collected seeds from Sarangani medicinal plants were sent to the National Plant Genetic Resources Laboratory of the University of the Philippines in Los Banos, Laguna for conservation purposes.
Results
Profile of the traditional healers
The demographic profiles of the traditional healers are presented in Table 2. Of the 12 traditional healers who consented to participate in the study, 5 were from Malapatan, 3 were from Alabel, and Glan and Maasim had 2 healers each. Female healers and those with B’laan ancestry predominated at 11 and 8, respectively, with 8 healers having no formal education and the rest having 1–6 years of primary education because of the distance of schools. Moreover, healers’ ages varied across a broad spectrum (27 to 110 years old), with a mean age of 63.9 years. In terms of healing experience, traditional practitioners ranged from being neophytes (1 year) to veteran healers (90 years), with most of them falling within the range of less than 20 years of experience. In terms of religion, the healers professed to be Christians, a fact borne out by small chapels established by Protestant missionaries from the lowlands. When asked about their sources of healing knowledge, all respondents received information through oral transmission, with ten healers learning from their parents and grandparents. The remaining healers availed of instruction from government-sponsored seminars or the radio. Unfortunately, a traditional healer refused to participate in an interview and disclose healing knowledge, as doing so could jeopardize her healing abilities.
Table 2. Demographic profiles of the traditional healers.
|
Demographic Profiles |
Details |
Frequency |
|
Gender |
Male |
8% |
|
Female |
92% |
|
|
Ethnicity |
B’laan |
67% |
|
T’boli |
17% |
|
|
Aklanon |
8% |
|
|
Lowland Tribes |
8% |
|
|
Education |
Primary |
36% |
|
Secondary |
0% |
|
|
Tertiary |
0% |
|
|
None |
64% |
|
|
Mean age |
63.9 |
|
|
Number of years practising healing |
≤ 20 years |
75% |
|
≥ 20 years |
25% |
|
|
Sources of healing knowledge |
Oral transmission |
83% |
|
Government-sponsored seminars/radio |
17% |
|
|
Perceived health status |
Healthy Sickly |
100% |
|
Religion |
Christian |
100% |
Moreover, the interviewed tribal healers disclosed that the ability to heal is a gift, and that it stays in the family. While most healers use plants alone to treat sick individuals, a few invoke the spirits through incantations.
Biodiversity assessment of Indigenous medicinal plants
A total of 39 IMP species were documented based on the accounts of the traditional healers (Table 3). However, only 32 species, belonging to 31 genera, 18 orders and 20 families, were collected during community walks. Seven taxa were identified up to the genus level only as they lack reproductive structures needed for species level identification. The comparable number of families and orders reflect the phylogenetic diversity of the medicinal plant species in the Sarangani upland communities. Families Asteraceae and Lamiaceae were the most represented with five species each. These were followed by families Euphorbiaceae, Moraceae, Poaceae and Zingiberaceae with two species each.
Of the collected plants, 26 were foraged within the community (backyards, roadsides and transition zones between forests and villages), while 6 species were collected in the forests by the healers. Moreover, of the 39 plant species identified by healers as having medicinal properties, 21% were trees, 56% were herbs, 5% were climbers or vines, and the remaining 18% were classified as shrubs or small trees.
Indigenous medicinal plants and traditional healing knowledge
From the semi-structured questionnaires and key informant interviews, information about the preparation and utilization of IMPs was collated. Most herbal remedies were prepared using primarily leaves (82%), while others used stems (or tree bark), roots, and plant sap. Moreover, traditional healers favoured decoction (85%) over fresh material use in their herbal concoctions. For some medicinal preparations, tree bark (or other tougher parts of the plant) was mixed with coconut oil and used as a liniment by spreading liberally on the skin. As for fresh leaves, some were directly applied to the skin as a poultice. Moreover, except for T’kulu (Tibouchina sp.), T’kas (Elytropappus sp.), Kataas (Colocasia esculenta (L.) Schott), K’lol (Tinospora crispa (L.) Hook. f. & Thomson), Langka (Artocarpus heterophyllus Lam.) and Luy-a (Zingiber officinale Roscoe), which were combined with other plants in coconut oil during the preparation of the herbal remedies, the remainder of the medicinal plants were given as single preparations.
Incidentally, the traditional healers did not have any concept of dosage and were not mindful of the proportions of plant parts to water or oil that they used in their preparations. Traditional healers likewise disclosed that most of the IMPs (56%) were readily available in the neighbourhood, did not need to be planted, and could be foraged anytime. Conversely, IMPs (predominantly trees and shrubs) found in the forests were less accessible, and their harvesting posed significant risks. Shown in Table 3 are the IMPs of the ethnic groups along with their scientific and local names, their habit, utilization and their availability in the upland areas of Sarangani Province.
Traditional healers in Sarangani Province classified human ailments into nine categories: (1) gastro-intestinal diseases, (2) head, ear, nose, and throat diseases, (3) cuts or wounds, (4) diseases of the bone and muscles, (5) urinary ailments, (6) cough/colds, (7) fever, (8) mouth/tongue/tooth problems and (9) other ailments (Table 3). In the upland areas, the more prevalent disorders were cough, loose bowel movement (LBM), kabuhi, stomachache and headache. A diagnosis of kabuhi is made when the patient experiences dizziness, nausea, chills and severe abdominal pain. This disorder is akin to heartburn, hyperacidity, or gastroesophageal reflux disease, depending on the nature and severity of symptoms. Furthermore, the healers revealed their capability to treat buyag, a culturally recognized ailment that can be loosely defined as a malady resulting from a curse imposed by someone with malevolent intent, an 'evil eye', or nature spirits. This supposed ailment necessitates incantations in addition to the IMPs.
Figure 2 shows some indigenous medicinal plants used by the traditional healers. As for their healing practices, traditional healers disclosed that decoctions of combined langka leaves/ ginger and Kataas/K’lol are effective against kabuhi. Among the T’bolis in Maasim, stems and leaves of T’kulu and T’kas are chopped into small pieces and put in a receptacle containing coconut oil. The resulting liniment or salve (haplas) is used to relieve shoulder pain and stomachache. For cough and colds, leaf decoctions of gabon (Blumea balsamifera), lagundi (Vitex negundo), mayana (Coleus scutellarioides), tawa-tawa (Euphorbia hirta), kalabo/balbas pusa (Orthosiphon aristatus) and mertaan (Ficus septica) are used by healers. For persons with LBM, root decoction of banlo-banlo (Galinsoga sp.) and leaf decoctions of star apple (Chrysophyllum cainito) and white flower (Andrographis paniculata) are given. In contrast, a tawa-tawa leaf decoction is given to a person suffering from headaches. On the other hand, patients with dengue are given papaya (Carica papaya) and tawa-tawa leaf decoctions, while fresh samples of mertaan, root decoctions of bulong baltang (Heliotropium indicum) and leaf decoctions of blibid (Eleusine indica) are given for bughat. Bughat, which loosely translates to relapse, is used to describe a condition when a person who is recovering from illness or who has shortly recovered from it becomes sick again. In addition, sili (Capsicum sp.) and tawal leaf decoctions are used to treat snake bites while gabon and galong are used for urinary tract infections by the traditional healers. To treat fever, healers use alingatong or Dendrocnide sp. (despite its itchiness), angelika/skaan bulan (Kalanchoe pinnata) and native sibuyas (Allium cepa). Regarding their utilization, tawa-tawa, kyama (Stevia rebaudiana) and mertaan have a wide range of medicinal uses. For instance, traditional healers use tawa-tawa for the treatment of malaria, cough, swelling, stomachache and headache, whereas kyama is utilized to address stomachache, toothache, dysmenorrhea, flatulence, and to facilitate wound cleansing. In addition, mertaan serves as a remedy for toothache, cough and bughat, while Coleus amboinicus, commonly referred to as oregano, is utilized for cough treatment and is widely utilized by the tribes. Moreover, another remarkable observation was related to plants having redundant utilities. For instance, tribal healers utilized ten, six, and five IMPs for common disorders like cough, LBM, and stomachache, respectively.
Table 3. Medicinal plants used in Sarangani Upland Communities. LBM, loose bowel movement; UTI, urinary tract infection; IUCN Categories: LC, least concern; EN, endangered; DD, data deficient.
|
Local Name |
English/ Common name |
Scientific name |
Family |
Order |
Used for |
Plant habit |
Plant part used |
Mode of preparation |
Mode of administration |
Where harvested |
Source |
Method of use |
Availability |
IUCN |
|
Alingatong |
Stinging nettle |
Dendrocnide sp. |
Urticaceae |
Rosales |
Fever |
Tree |
Leaf |
Decoction |
Drunk |
Collected from the wild |
Wild-harvested |
Singly |
Less available |
|
|
Ampalaya |
Bitter gourd |
Mimordica charantia |
Cucurbitaceae |
Cucurbitales |
Cough |
Climber |
Leaf |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Readily available |
|
|
Angelika / Skaan Bulan |
Katakataka / Air plant / Cathedral bells |
Kalanchoe pinnata (Lam.) Pers. |
Crassulaceae |
Saxifragales |
Fever; Cough |
Herb |
Leaf |
Decoction; Fresh |
Drunk; External/ rubbing |
Home garden |
Cultivated |
Singly |
Less available |
|
|
Avocado |
Avocado |
Persea americana Mill. |
Lauraceae |
Laurales |
LBM |
Tree |
Leaf |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Readily available |
LC |
|
Banlo-banlo |
Gallant soldier |
Galinsoga sp. |
Asteraceae |
Asterales |
LBM |
Herb |
Root |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Readily available |
|
|
Blilid |
Goose Grass |
Eleusine indica (L.) Gaertn. |
Poaceae |
Poales |
Bughat (Relapse) |
Herb |
Leaf |
Decoction |
Drunk |
Ubiquitous |
Wild-harvested |
Singly |
Less available |
LC |
|
Bulong baltang |
Indian heliotrope |
Heliotropium indicum L. |
Boraginaceae |
Boraginales |
Bughat (Relapse) |
Herb |
Root |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Readily available |
|
|
Gabon |
Sambong |
Blumea balsamifera (L.) DC. |
Asteraceae |
Asterales |
Cough; UTI |
Shrub |
Leaf |
Decoction |
Drunk |
Collected from the Wild; Home garden |
Wild-harvested; Cultivated |
Singly |
Readily available |
LC |
|
Galong |
Stomachache; UTI2; Jaundice |
Tree |
Leaf |
Decoction |
Drunk |
Collected from the wild |
Wild-harvested |
Singly |
Less available |
|||||
|
Kalabo / Balbas pusa |
Cat’s whiskers |
Orthosiphon aristatus (Blume) Miq. |
Lamiaceae |
Lamiales |
Cough; Cold |
Herb |
Leaf |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Less available |
|
|
Kape |
Coffee |
Coffea arabica L. |
Rubiaceae |
Rubiales |
LBM |
Shrub |
Leaf |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Readily available |
EN |
|
Kataas |
Taro |
Colocasia esculenta (L.) Schott |
Araceae |
Alismatales |
Kabuhi (Heartburn) |
Herb |
Leaf |
Fresh |
External/ rubbing |
Collected from the wild |
Wild-harvested |
With other plant |
Less available |
LC |
|
K’lol |
Makabuhay |
Tinospora crispa (L.) Hook.f. & Thomson |
Menispermaceae |
Ranunculales |
Kabuhi (Heartburn) |
Climber |
Root |
Fresh |
External/ rubbing |
Collected from the wild |
Wild-harvested |
With other plant |
Less available |
|
|
Kusol |
Aromatic ginger |
Kaempferia galanga (L.) |
Zingiberaceae |
Zingiberales |
Earache |
Herb |
Leaf |
Fresh |
Ear Drops |
Home garden |
Cultivated |
Singly |
Less available |
DD |
|
Kyama |
Candy leaf |
Stevia rebaudiana (Berdoni) Berdoni |
Asteraceae |
Asterales |
Stomachache; toothache; Wound cleaning; Dysmenorrhea; Flatulence |
Herb |
leaf |
Decoction |
Drunk |
Collected from the wild |
Wild-harvested |
Singly |
Less available |
|
|
Lagano |
Oregano |
Coleus amboinicus Lour. |
Lamiaceae |
Lamiales |
Cough |
Herb |
Leaf |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Readily available |
|
|
Lagundi |
Lagundi |
Vitex negundo L. |
Lamiaceae |
Lamiales |
Cough |
Shrub |
Leaf |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Readily available |
LC |
|
Langka |
Jackfruit |
Artocarpus heterophyllus Lam. |
Moraceae |
Rosales |
Kabuhi (Heartburn) |
Tree |
Leaf |
Decoction |
Drunk |
Collected from the wild |
Wild-harvested |
With other plant |
Readily available |
|
|
Layet langas |
Headache; LBM |
Herb |
Leaf |
Decoction |
Drunk |
Ubiquitous |
Wild-harvested; Cultivated |
Singly |
Less available |
|||||
|
Luy-a |
Ginger |
Zingiber officinale Roscoe |
Zingiberaceae |
Zingiberales |
Kabuhi (Heartburn) |
Herb |
Stem |
Decoction |
Drunk |
Collected from the wild; Home garden |
Wild-harvested; Cultivated |
With other plant |
Readily available |
DD |
|
Mayana |
Coleus |
Coleus scutellarioides (L.) Benth. |
Lamiaceae |
Lamiales |
Cough |
Herb |
Leaf |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Readily available |
|
|
Mertaan |
Fig tree |
Ficus septica Burm. f. |
Moraceae |
Rosales |
Toothache; Cough; Relapse |
Shrub |
Leaf |
Fresh |
Poultice |
Collected from the wild |
Wild-harvested |
Singly |
Less available |
LC |
|
Nabol |
Tongue Sore |
Tree |
Sap |
Fresh |
Home garden |
Cultivated |
Singly |
Readily available |
||||||
|
Native sibuyas |
Onion |
Allium cepa L. |
Amaryllidaceae |
Asparagales |
Fever |
Herb |
Leaf |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Readily available |
|
|
Papaya |
Papaya |
Carica papaya L. |
Caricaceae |
Brassicales |
Dengue |
Tree |
Leaf |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Readily available |
DD |
|
Sili |
Sili |
Capsicum sp. |
Solanaceae |
Solanales |
Snake Bite |
Herb |
Leaf |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Readily available |
|
|
Sislok |
Wound Cleaning |
Herb |
Leaf |
Fresh |
Poultice |
Ubiquitous |
Wild-harvested; Cultivated |
Singly |
Less available |
|||||
|
S’lot |
Carabao grass |
Paspalum conjugatum P.J. Bergius |
Poaceae |
Poales |
Vomiting |
Herb |
Leaf |
Decoction |
Drunk |
Ubiquitous |
Wild-harvested; Cultivated |
Singly |
Less available |
LC |
|
Star apple |
Star apple |
Chrysophyllum cainito L. |
Sapotaceae |
Ericales |
LBM |
Tree |
Leaf |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Readily available |
LC |
|
Talil |
Vomiting |
Herb |
Stem |
Decoction |
Drunk |
Collected from the wild |
Wild-harvested |
Singly |
Less available |
|||||
|
Tambisan |
Mugwort |
Artemisia sp. |
Asteraceae |
Asterales |
Cough |
Herb |
Leaf |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Readily available |
|
|
Tawal |
Snake Bite |
Tree |
Leaf |
Decoction |
Drunk |
Collected from the wild |
Wild-harvested |
Singly |
Readily available |
|||||
|
Tawa-tawa |
Asthma plant |
Euphorbia hirta L. |
Euphorbiaceae |
Malpighiales |
Malaria; Cough; Swelling; Stomachache; Headache |
Herb |
Leaf; root |
Decoction |
Drunk |
Collected from the wild; Home garden |
Wild-harvested; Cultivated |
Singly |
Less Available |
|
|
T’kas |
Elytropappus sp. |
Asteraceae |
Asterales |
Shoulder pain |
Shrub |
Stem |
Decoction |
Drunk |
Collected from the wild |
Wild-harvested |
With other plant |
Less Available |
||
|
T’kulu |
Tibouchina sp. |
Melastomataceae |
Myrtales |
Shoulder pain |
Shrub |
Leaf |
Decoction |
Drunk |
Collected from the wild |
Wild-harvested |
With other plant |
Less Available |
||
|
Tuba-tuba |
Tubang bakod |
Jatropha curcas L. |
Euphorbiaceae |
Malpighiales |
Mouth sore; Headache |
Shrub |
Leaf |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Readily available |
LC |
|
Vicks Sibu |
Mint |
Mentha sp. |
Lamiaceae |
Lamiales |
Fever; Cough |
Herb |
Leaf |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Readily available |
|
|
White flower |
Green Chiretta |
Andrographis paniculata (Burm. f.) Wall. ex Nees |
Acanthaceae |
Lamiales |
LBM |
Herb |
Leaf |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Readily available |
|
|
Wuh |
Toothache |
Herb |
Leaf |
Decoction |
Drunk |
Home garden |
Cultivated |
Singly |
Readily available |
Indigenous medicinal plants: threats and conservation initiatives

Questionnaire administration and in-depth conversations with key informants were carried out to ascertain threats to their medicinal plant resource base. Figure 3 illustrates the challenges traditional healers encounter in the Sarangani uplands about their THK and the IMPs they utilize. The cultural practice of swiddening or alnigo (Figure 3a) before upland rice cultivation led to significant deforestation and considerable biodiversity losses (Figure 3c). Another legitimate concern raised by the locals during field observations was the considerable deforestation caused by unregulated resource extraction in the mountainous regions. Figure 3b, conversely, depicts an elderly tribal healer who has surpassed the remarkable age of 100 years but who was still active on the farm. Regrettably, these elderly healers expressed their sorrow over their failure to pass on THK to the younger generation, attributing this to a notable disinterest from the latter.
Upon the demise of these knowledge keepers, the invaluable information they possess will be irretrievably lost to humanity. Finally, the waning interest of the younger generation in traditional healing and their preference for modern medicines (Figure 3d) were also identified as significant threats to the perpetuation of traditional healing practices and the conservation of IMPs. Conversations with tribal healers indicated that although certain medicinal plants could be harvested year-round from home gardens and forest fringes, other IPMs were diminishing due to various stresses.
From 2016 to 2017, the prolonged effects of El Niño resulted in wide-scale losses of flora in the Sarangani uplands. Other threats identified by the healers were climate change-related devastation (such as heavy rains and flash floods), pest infestation, unregulated harvesting, forest denudation, and the shift to modern medicines. The healers also disclosed that they had to walk long distances to harvest rarely occurring medicinal plants previously abundant in the communities. Moreover, residents from relatively accessible settlements such as Lamlifew (Malungon) and Sitio Malaya (Kiamba) disclosed that they forsook traditional remedies in favour of modern medicines several years back, owing to the perceived superiority of the latter. Furthermore, the healers acknowledged the potential extinction threats of medicinal plants if conservation efforts are not implemented. Through continuous cultivation of IMPs in their backyards and home gardens, the healers inadvertently conserved these invaluable genetic treasures. Furthermore, the healers disclosed that to avert the extinction of IMPs in their natural habitats, they exclusively harvest what is necessary.
Discussion
Sarangani traditional healers: A dying breed?
One important feature of the Sarangani traditional healthcare system is the preponderance of female healers – a fact that emphasizes their vital roles in the traditional healing system. This association of women with traditional healing practices transcends cultures due to their nurturing nature and profound knowledge of plants that thrive in their communities. Struthers (2003) reported that Aboriginal women healers in the United States and Canada generally practised holistic healing using age-old methods passed down by their ancestors. However, the idea that women are the predominant healers is not a universal truth, as there are cultures where male healers serve as the primary practitioners (Gessler et al, 1995; Semenya and Potgieter, 2014). In Morocco, Bakker (1992) documented the notable rise of Berber women as traditional healers when their male counterparts lost influence due to political upheavals in the region. French colonization and the consequent succession of the Moroccan Makhzen in the political sphere stripped male healers of prestige, leading to the remarkable emergence of women healers to fill this healthcare vacuum. This is one case wherein politics, and not modernization, was the identified cause of shifting gender roles in the traditional healthcare system. Another study about Busoga healthcare practitioners in Uganda (Isiko, 2018) revealed that while men and women are equally accepted in traditional medicine, the power and influence that they wield depend on societal expectations relating to gender roles.

Figure 3. Threats to medicinal plants and traditional healing knowledge in the Sarangani uplands: a, ongoing Alnigo (or swiddening); b, advanced ages of knowledge keepers and non-transmission of healing knowledge to succeeding generations; c, denudation of mountains; d, proliferation of modern medicines.
It must likewise be emphasized that traditional healers possess a critical understanding of medicinal plants, owing to their long years of experimentation and use. Acquiring and mastering utilization of such material requires significant time and effort. This knowledge, transmitted to them through generations, enables them to provide healing and therapy for poverty-stricken communities beyond the reach of basic social services. However, one factor that does not bode well for the perpetuation of traditional knowledge was the advanced ages of the Sarangani knowledge keepers. Similarly, Teves et al (2023) reported that Eskaya healers in Bohol, Philippines, are dwindling in numbers because of old age-related deaths. These are elderly people who become weak and decrepit with advancing years, lack of proper nutrition and inadequate health care due to the remoteness of their villages. Moreover, traditional healing knowledge, being passed on to chosen members of the family, limits its transmission, especially when the appointed successor does not show any interest in learning these skills. Consequently, when these elderly healers pass on, the priceless healing knowledge that they possess will forever be lost to humanity.
Sarangani Indigenous medicinal plants: Current state and major pressures
This study revealed a significant number of IMPs and a diverse repertoire of healing rituals and knowledge among the visited ethnic communities in the Sarangani uplands. This prevalent use of medicinal plants for healing in other areas of Mindanao has been reported in the Mount Matutum Protected Landscape (Alinsug et al, 2022), Agusan del Sur (Dapar et al, 2020), Davao Occidental (Paraguison et al, 2020; Cabugatan et al, 2022) and Surigao del Sur (Ilagan et al, 2022). Community inventory also revealed that Sarangani medicinal plants with high utilization were more frequently found closer to home. This fact underscores the direct correlation between the availability and cultural importance of medicinal plants to the Sarangani tribes. With greater accessibility, healers have more opportunities to test by trial and error the efficacy of potentially medicinal plants (Vandebroek et al, 2008). Furthermore, in Sarangani upland tribal communities, a direct relationship between the redundancy of medicinal plant use and the more prevalent physical ailments was established. This relationship was likewise borne out by studies done by Kunwar et al (2015), Kumar and Bussman (2011), and Vandebroek et al (2008) in Nepal, India, and Bolivian Andes, respectively.
However, during recent years, the multi-fold effects of rapidly evolving social-ecological scenarios have severely impacted the Sarangani traditional agroecosystem, resulting in wide-scale natural resource losses. Moreover, species introductions from the lowlands resulted in a mosaic of Indigenous and non-indigenous medicinal plants, giving the healers a more expansive repertoire on which to experiment. Study results revealed, however, that IMPs (especially those thriving in the wild) are declining in terms of numbers in their natural habitats. Among the identified pressures leading to these losses are climate change-related devastation (such as heavy rains and flash floods), pest infestation, unregulated harvesting and forest denudation. In addition, IMPs thriving in transition areas and roadsides are more often subjected to anthropogenic pressures, resulting in their diminished numbers. While some IMPs are still available, several could no longer be found in the vicinity, and tribal healers reported travelling long distances to harvest them. In Limpopo Province, South Africa, locals identified over-harvesting and indiscriminate collection of IMPs as factors leading to large-scale losses (Mathibela et al, 2015). Moreover, several studies in Sri Lanka and Northern Ethiopia ascribe losses of IMPs to ecological devastation, climate change-associated devastation, agricultural expansion and human habitation, among other factors (De Silva and Wettasinghe, 2004; Mesfin et al, 2013). Owing to the burgeoning global population, the increased demand for modern medicines as well as the international trade for medicines by pharmaceutical companies, IMPs are disappearing in the wild because of overharvesting (Soetan and Aiyelaagbe, 2009; Oladele et al. 2011; Otieno and Analo, 2012; Ganie et al. 2015). Another study by Birhanu et al (2015) identified the shift to modern medicines as a factor leading to the extinction of IMPs. In the Sarangani uplands, conversations with locals revealed the use of modern medicines, such as paracetamol (for headaches), loperamide (for LBM), phenylephrine HCL or Neozep (for colds), Bioflu (colds and flu) and mefenamic acid (toothache). To prevent infection, tribal people open an amoxicillin capsule and sprinkle its contents on an open wound.
Accessibility of the tribal communities was also identified as a factor contributing to medicinal plant losses in the Sarangani uplands. Villages like Lamlifew (Malungon) and Sitio Malaya (Kiamba) are relatively accessible and can be reached by 4x4 vehicles and single motorcycles. The former community is dominated by B’laans and is frequently frequented by tourists and researchers for its School of Living Tradition for abaca weaving. Local inhabitants of Lamlifew enjoy the creature comforts of modernization (i.e. running water, electricity, cellphone service, internet service and cable television, among others). Sitio Malaya, on the other hand, is inhabited by T’bolis who manage a thriving abaca industry for local and international markets. All household needs (food and medicines) are purchased from the lowland markets. In both these places, traditional healing had been wholly abandoned for modern medicine. In a study done in the Himalayas, Tali et al (2014) identified agricultural expansion, road improvement, overgrazing and deforestation as threats leading to the extinction of medicinal plants. Furthermore, increased accessibility and foreign introductions resulted in a mosaic of Indigenous and non-indigenous medicinal plants in the Sarangani ethnic communities, resulting in a more diversified pharmacopoeia. Needless to say, medicinal plants remain the sole refuge of remote tribal communities in Sarangani Province, where the provision of basic social services is scanty at best and non-existent at worst. The need for self-sufficiency was highlighted during the COVID-19 pandemic (2019–2021) when these communities were isolated, travel was prohibited, food/resource supply chains were disrupted, and prices of commodities soared beyond the reach of many.
Furthermore, the practice of traditional healing was more prevalent in rural communities with very little/no access to modern medicines owing to geographical isolation and economic reasons (Maramba-Lazarte, 2020). In another study done in six middle-income countries (China, Ghana, India, Mexico, Russia and South Africa), Oyebode et al (2016) identified factors leading to the decline in the use of medicinal plants in these countries. These were the significant shifts in social trends and cultural beliefs, as well as the political support and provision of resources for training, practising and increasing public awareness of modern medicines.
Traditional healing knowledge: Headed for oblivion
In the remote Sarangani uplands, conversion to Christianity primarily resulted in the abandonment of belief in nature spirits. For some healers, however, some vestiges of spiritism persisted. In fact, this belief that human activities intersect with the goings-on in the spiritual world persists even with the incursion of modernization and Christianization. Similarly, local inhabitants in Namibia, South Africa and Bangladesh believe that nature spirits influence their health and that the efficacy of IMPs hinges on a complete understanding of their physical and spiritual purposes (Motaleb et al, 2010; Cheikhyoussef et al, 2011; Stofferson et al, 2011). This persistence of spiritism in healing practices, which has been labelled as pagan and backwards, has caused a significant number of Sarangani locals to forsake traditional medicine for modern medicine.
In the Sarangani uplands, losses of THK can be ascribed to additional pressures such as acculturation, education, increasing accessibility of the communities, the lure of modernization/technology, aging knowledge keepers (healers) and the oral nature of knowledge transmission that predisposes it to loss (Posey, 1996). Mahwasane et al (2013) concurred that the THK is gradually becoming extinct in the absence of a writing system and because healers do not keep written records. In South Africa, THK has been largely ignored because, being verbally transmitted, it could not be included in school curricula or policy documents (Mathibela et al, 2015). Consequently, huge volumes of THK worldwide remain undocumented, thereby underscoring now more than ever the need to record THK and conserve IMPs, before they completely disappear. In addition, the unwillingness of some healers (particularly in Kiamba and Maitum) to divulge healing knowledge that they consider secret information likewise exacerbates THK losses. This unwillingness to share THK was also reported by Kala et al (2006) and Giday et al (2003). Others are wary about researchers coming to their communities and extracting traditional knowledge that had been passed on to them by their ancestors. The lack of written records due to the oral nature of knowledge transmission compounds these losses, while the secretive nature of some healers dooms knowledge transmission to permanent loss.
Further exacerbating these losses is the diminished intergenerational knowledge transfer of THK. Consequently, there is no mentoring for the next generation and, if the elderly healers pass on, their THK will be lost forever. In the Sarangani uplands, THK is losing its appeal among the younger generation, who consider these as backward, primitive, unchristian and inferior to modern medicine. In rural Malaysia, the oral nature of mentoring has also caused failure in THK transmission to the next generation (Batugal et al, 2004). Consequently, the older generation of healers will have no pool of recruits to inherit their knowledge and practices. Further contributing to the decline in the practice of THK is the proliferation of private and state-sponsored health facilities all over the province, especially in more accessible areas.
Future directions
Sarangani traditional healthcare system: Ways forward
In Sarangani Province, healers’ knowledge results from learning and social interactions between knowledge keepers and those who seek it. However, the majority of THK practitioners still lack scientific justifications for their methodologies. Although they believe in the outcomes of their practices, they lack understanding of the mechanisms that produce these effects. Interviewed healers were unable to elucidate the mechanisms and efficacy of the remedies.
Bannerman (1977) emphasized the necessity of assessing THK through the lens of contemporary science, thereby enhancing beneficial practices and safeguarding against detrimental ones. Rather than depending on trial and error resulting from arbitrary screening methods, well-documented THK could assist scientists in identifying plants with potential medical characteristics. Scientific validation of IMPs through phytochemical, toxicological and pharmacological studies is thus warranted to eliminate quackery associated with THK, warn against inappropriate usage, and identify potential sources of medicines. However, one crucial matter that needs to be considered is the lack of coherence among healers about modes of preparation and proper dosages of IMPs (Wilcox and Bodeker, 2004). Once the effectiveness of THK is properly assessed, the next logical step is its integration into a nation’s healthcare delivery system.
Integrating THK into national healthcare will preserve the Indigenous peoples’ cultural heritage for future generations (Mahwasane et al, 2013). One way to do this is by including traditional healers in the crafting of a comprehensive healthcare strategy that is grounded in inclusivity, knowledge pluralism and sharing of information. In 1997, the Philippine government passed the Traditional and Alternative Medicine Act, which affirmed government support for THK (Maramba-Lazarte, 2020). Kaido (1997) proposed that traditional healers could be significantly used if they were organized and trained. Empowering traditional healers to participate in the crafting of local healthcare strategies for disadvantaged people whose views are oftentimes ignored during deliberations is also suggested. Moreover, policy positions relating to THK promotion should be more nuanced, and the use of IMPs must not be encouraged when there are reasons to doubt their effectiveness in comparison to modern medicine. Ultimately, collaborative initiatives by the scientific community and governments are essential to generate the impetus for such actions. Dissemination of pertinent research findings and facilitating further education and training programmes for traditional healers will empower them to document and share their significant Indigenous knowledge independently. The use of audiovisual media, espoused by Bidwell et al (2011), can serve as an effective means for knowledge transfer.
Biocultural conservation
A comprehensive inventory of IMPs must be undertaken before any conservation initiative commences. Soetan and Aiyelaagbe (2009) stated that IMPs, when not recorded or classified, can hamper conservation efforts. The importance of documenting IMPs as a prelude to their conservation was also espoused by Hamilton (2003). In the Sarangani upland communities, emerging sociocultural scenarios underscore the need for complementary ex situ and in situ conservation of IMPs. Through continuous utilization and cultivation of IMPs in their backyards and home gardens, the healers are unknowingly conserving these priceless genetic resources. The healers also practice judicious collection of IMPs and only harvest when these are needed. In a rural Nigerian community, Oladele et al (2011) reported that the cultivation of IMPs contributed to their conservation while Batugal et al (2014) espoused continuous cultivation as an efficient conservation strategy. In Africa, Okigbo et al (2008) maintained that only through sustainable conservation practices can a constant supply of IMPs be ensured for prolonged periods.
In Southern Italy, regional and national parks (considered protected areas) that feature medicinal plants conserved ex situ attract ethnobotanists from all over the country because of the joint preservation of IMPs and associated THK of the rural people (Menale et al, 2016). Along these lines, community-initiated ex situ conservation of Sarangani IMPs and THK must be undertaken in collaboration with academia, the local government and other stakeholders to preclude further losses of IMPs. In doing this, priority should be given to IMPs having redundant utilities since this will help offset pressure on IMPs that are considerably threatened in the wild.
As for the IMPs collected in the Sarangani uplands, these were sent to the Philippine national genebank for ex situ conservation. This backup collection will serve as an ‘insurance policy’ against the extinction of medicinal plant species amidst widespread environmental devastation in their natural habitats in the Sarangani uplands. Additionally, these IMPs are potential sources of new drugs for present and future health needs, not just of the locals but also of the communities at large. The need to preserve THK via knowledge transfer is crucial for the perpetuation of tribal culture and the promotion of local communities' rights over their plant genetic resources. Moreover, THK, when harmonized with frontier knowledge, may prove useful in addressing problems that may arise in the future. Recognizing the significance of the knowledge held by these healers and meticulously recording essential elements with sensitivity and respect for intellectual property rights are paramount in assisting the healers (Mathibela et al, 2015). Therefore, it is important to have a governance framework to effectively protect the THK of the tribes for posterity.
Limitations of the study
This study covered a limited number of study sites and gleaned valuable healing knowledge from a handful of traditional healers. Some of the sitios were inaccessible due to geographic isolation and difficult terrain, while others, unfortunately, still experience peace and order issues brought by insurgent groups, specifically in the towns of Banlas, Malapatan, Datal Anggas and Alabel. In addition, the danger posed by armed jihadist Muslim groups also prevented the research team from exploring areas in Maasim and Maitum. As for the healers themselves, some were unwilling to share healing knowledge in the belief that doing so would diminish their powers, while others were wary about sharing traditional knowledge with outsiders who they believe are merely out to extract information from them. Moreover, in some sitios, the locals had completely shifted to modern medicine and traditional healers were nowhere to be found. Furthermore, on the part of the researchers, the expensive and lengthy process of securing government permits for every community visited often discourages them from visiting more communities. Consequently, as some of the healers did not impart their THK, it is possible that some of the IMPs were not documented in this study.
Conclusion
This study unveiled the healing knowledge of local healers and the diversity of medicinal plants in the Sarangani uplands. Results, however, revealed that these IMPs are declining in numbers because of environmental degradation and the shift to modern medicines, among other pressures. Also revealed by this study are THK losses due to the advanced ages of knowledge keepers and the shifting preferences of the Sarangani locals towards modern medicine. To preclude further losses of IMPs, the following are recommended: (1) complementary in situ and ex situ conservation, (2) rehabilitation of the natural habitats of IMPs, (3) documentation of the THK of elderly healers before they pass on, (4) further scientific studies to validate THK, (5) establishment of a school of living traditions for the preservation of THK and its transmission to the younger generation, (6) protection of IMPs from exploitation and biopiracy through appropriate policy and legislation and (7) promotion of value-adding, utilization and widescale cultivation of IMPs. Having a continuous supply of IMPs (along with their associated traditional knowledge) to promote and support the health of the locals will bring the community (and eventually the Philippines) closer to the attainment of its Sustainable Development Goals (SDGs), such as improved health (SDG3), empowerment of the tribal women (SDG5), and self-sustainability (SDG11) in the face of disasters and isolation. Furthermore, when validated by scientific knowledge and promoted, these IMPs can be a potential livelihood source for tribal households, resulting in improved household income. Through these interventions, it is envisaged that the Sarangani IMPs and their associated THK will be preserved for future generations of tribes. Finally, the conservation of THK will likewise make tribal households more resilient against the ravages of climate change, pandemics, and other future problems and perturbations.
Traditional healers’ organization, empowerment and participation are essential for developing suitable and culturally sensitive healthcare interventions for the local community.
Supplemental Material 1. Questionnaire about Sarangani Indigenous medicinal plants
Acknowledgments
The authors extend their most profound thanks to the tribal healers who took part in the study.
Authors’ contributions
FLZ conceptualized the study, supervised its implementation, revised the first draft, and co-wrote the final paper with MCBH, who also carried out confirmation of taxonomic identification of medicinal plants and finalization of the article. BMGB carried out the majority of field work, wrote the first draft and did data analysis. CRMR provided good quality pictures for the paper, helped in field collection and in the processing of the paper for publication while CHMA assisted in field preparations, collection and ex situ conservation of collected medicinal plants at the Philippine National Genebank.
Conflict of interest statement
The authors have declared that no competing interests exist.
Ethics statement
A free and prior informed consent for this study was incorporated in the application sent to the National Commission on Indigenous Peoples (NCIP) by Sarangani Province as part of its ‘Ridge to Reef’ project funded by the Peoples’ Survival Fund.
References
Agduma, A.R., Garcia, F.G., Cabasan, M.T., et al, 2023. Overview of priorities, threats, and challenges to biodiversity conservation in the southern Philippines. Reg. Sustain 4, 203e213. https://doi.org/10.1016/j.regsus.2023.05.003
Alinsug, M.V., Estandarte, M.H.G., Somodio, E.M.N., Sabarity, M.J.J., Deocaris, C.C., 2022. Biodiversity of ethnomedicinal plants from the B’laan tribe in Mount Matutum Protected Landscape, Southern Mindanao, Philippines. Biodiversitas, 23:1, 554-563. https://doi.org/10.13057/biodiv/d230160
Ambasta, S.K., Kumari, S., Yadav, A.K., Trivedi, I., Prasad, B., Sinha, U.K., 2016. Medicinal plants of Bihar and its neighboring region which needs attention for their conservation. European Journal of Biomedical and Pharmaceutical Sciences, 3(4), 554-550. https://www.researchgate.net/publication/327210058_medicinal_plants_of_Bihar_and_its_neighboring_region_which_needs_attention_for_their_conservation
Aryal, K.K., Dhimal, M., Pandey, A., Pandey, A.R., Dhungana, R., Khaniya, B.N., Mehta, R.K., Karki, K.B., 2016. Knowledge Diversity and Healing Practices of Traditional Medicine in Nepal. Kathmandu, Nepal: Nepal Health Research Council. https://www.researchgate.net/publication/313159390_Knowledge_Diversity_and_Healing_Practices_of_Traditional_Medicine_in_Nepal
Bakker, J., 1992. The Rise of female healers in the Middle Atlas, Morocco. Social Science and Medicine, 35(6); 819-829. https://doi.org/10.1016/0277-9536(92)90082-2
Bankole, A. E., Adekunle, A. A., Sowemimo, A. A., Umebese, C. E., Abiodun, O., Gbotosho, G. O., 2015. Phytochemical screening and in vivo antimalarial activity of extracts from three medicinal plants used in malaria treatment in Nigeria. DOI https://doi.org/
Bannerman, R.H., 1977. WHO’s programme: the approach will focus on the psychosocial and anthropological aspects of traditional medicine, on acupuncture and other healing methods, and on the claims made for herbs and medicinal plants. World Health, (November, 16-17). World Health Organization. https://iris.who.int/handle/10665/326066
Barata, A.M., Rocha, F., Lopes, V., Carvalho, A. M., 2016. Conservation and sustainable uses of medicinal plants and aromatic plants genetic resources on the worldwide for human welfare. Industrial Crops and Products. https://doi.org/10.1016/j.indcrop.2016.02.035
Batugal, P.A., Kanniah, J., Sy, L., Oliver, J.T., 2004. Medicinal plants research in Asia, Volume 1: The framework and project workplans. International Plant Genetic Resources Institute – Regional Office for Asia, the Pacific and Oceania (IPGRI-APO), Serdang, Selangor DE, Malaysia. ISBN 929043-615-8. https://cgspace.cgiar.org/server/api/core/bitstreams/edad56b4-e6ce-4c1e-9328-8eb4f0fe1d33/content
Belgica, T.H.R., Suba, M.D., Alejandro, G.J.G., 2024. Botanical assessment and conservation status of medicinal plants in mountain range of Malinao Albay, Philippines. Biodiversitas, 25:4, 1413-1419, DOI: https://doi.org/
Bidwell, N.J., Winschiers-Theophilus, H., Koch Kapuire, G., & Chivuno-Kuria, S., 2011. Situated interactions between audiovisual media and African herbal lore. In Proceedings of the 2nd ACM SIGCHI Workshop on Walking Together to Design (pp. 1-4). ACM. https://doi.org/10.1007/s00779-010-0337-1
Birhanu, T., Abera, D., Ejeta, E., 2015. Ethnobotanical study of medicinal plants in selected Horro Gudurru Woderas, Western Ethiopia. Journal of Biology, Agriculture and Healthcare. ISSN 2224-3208. https://www.researchgate.net/publication/279512308_Ethnobotanical_Study_of_Medicinal_Plants_in_Selected_Horro_Gudurru_Woredas_Western_Ethiopia
Borokini, T.I., Ighere, D.A., Clement, M., Ajiboye, T.O., Alowonle, A.A., 2013. Ethnobiological Survey of Traditional Medicine Practice for Women’s Health in Oyo State. Journal of Medicinal Plants Studies, 1(5): 17-29. https://www.plantsjournal.com/archives/2013/vol1issue5/PartA/2.1.pdf
Cabugatan, M.A.D., Ong, R.L.J.T., Mancao, L.S., et al, 2022. Ethnobotanical survey on medicinal plants used by the Manobo tribe of Don Marcelino, Davao Occidental, Philippines. Asian Journal of Biological and Life Sciences, 11, 492e504. https://doi.org/10.5530/ajbls.2022.11.67
Cheikhyoussef, A., Shapi, M., Matengu, K., Ashekele, H. M., 2011. Ethnobotanical study of indigenous knowledge on medicinal plant use by traditional healers in Oshikoto region, Namibia. Journal of Ethnobiology and Ethnomedicine. https://ethnobiomed.biomedcentral.com/articles/10.1186/1746-4269-7-10
Convention on Biological Diversity (CBD). Philippines - Country Profile. Biodiversity Facts: Status and trends of biodiversity, including benefits from biodiversity and ecosystem services. https://www.cbd.int/countries/profile?country=ph
Cordero, C.S., Meve, U., Alejandro, G.J.D., 2022. Ethnobotanical documentation of medicinal plants used by the indigenous Panay-Bukidnon in Lambunao, Iloilo, Philippines. Frontiers in Pharmacology, 12, 1-20. doi: https://doi.org/
Cotton, C. M., 1996. Ethnobotany: Principles and applications. Chichester, England: John Wiley and Sons. https://doi.org/10.1021/JM9701841
Dapar, M.L.G., Alejandro, G.J.D., Meve U., Liede-Schumann, S., 2020. Quantitative ethnopharmacological documentation and molecular confirmation of medicinal plants used by the Manobo tribe of Agusan del Sur, Philippines. Journal of Ethnobiology and Ethnomedicine, 16:14. https://doi.org/10.1186/s13002-020-00363-7.
De Silva, M. A., Wettasinghe D. T., 2004. Sri Lanka conservation and sustainable use of medicinal plants. IUCN – The World Conservation Union Sri Lanka. https://iucn.org/sites/default/files/2022-05/sri_lanka_conserv_sustain_use_med_plants.pdf
Fiscal, R.R., 2017. Ethnomedicinal plants used by the traditional healers in Laguna, Philippines. Asia Pacific Journal of Multidisciplinary Research, 5(4), 132-137. https://www.researchgate.net/publication/322929882_Ethnomedicinal_Plants_Used_by_Traditional_Healers_in_Laguna_Philippines
Ganie, S. H., Upadhyay, P., Das, S., Sharma, M.P., 2015. Authentication of medicinal plants by DNA markers. Plant Gene, 4, 83-99. https://doi.org/10.1016/j.plgene.2015.10.002
Gessler, M.C., Msuya, D.E., Nkunya, M.H.H., Schir, H.M., Tanner, M., 1995. Traditional healers in Tanzania: Socio-cultural profile and three short portraits. Journal of Ethnopharmacology, 48, 145-160. https://pubmed.ncbi.nlm.nih.gov/8719975/
Giday, M., Asfaw, Z., Elmqvist, T., Woldu, Z., 2003. An ethnobotanical study of medicinal plants used by the Zay people in Ethiopia. Journal of Ethnopharmacology, 85(1):43–52. PMID: 12576201. https://pubmed.ncbi.nlm.nih.gov/12576201/
Hamilton, A., 2003. Medicinal plants, conservation and livelihoods. Biodiversity and Conservation, 13: 1477-1577. https://www.researchgate.net/publication/227147775_Medicinal_Plants_Conservation_and_Livelihoods
Ilagan, V.A.D., Alejandro, G.J.D., Paraguison, D.J.B., et al., 2022. Ethno-pharmacological documentation and molecular authentication of medicinal plants used by the Manobo and Mamanwa tribes of Surigao del Sur, Philippines. Biodiversitas, 23, 3185e3202. https://doi.org/10.13057/biodiv/d230646
Isiko, A.P., 2018. Gender roles in traditional healing practices in Busoga. Retrieved from https://hdl.handle.net/1887/63215
Kaido, T.L., Veale, J.H., Havlika, I., Rama, B.K., 1997. Preliminary screening of plants used in South Africa as traditional herbal remedies during pregnancy and labour. Journal of Ethnopharmacology, 55, 145-160. https://pubmed.ncbi.nlm.nih.gov/9080339/
Kala, C.P., Dhyani, P.P., Sajwan, B.S., 2006. Developing the medicinal plants sector in northern India: challenges and opportunities. Journal of Ethnobiology and Ethnomedicine, 2:32. https://ethnobiomed.biomedcentral.com/articles/10.1186/1746-4269-2-32
Kumar, M., Bussmann, R.W., 2011. Ethnomedicinal and ecological status of plants in Garhwal Himalaya, India. Journal of Ethnobiology and Ethnomedicine, BioMed Central Ltd; 7(1):32. Available from: http://www.ethnobiomed.com/content/7/1/32
Kunwar, R., Acharya, R.P., Chaodhary, C.L., 2015. Medicinal plant dynamics in indigenous medicines in farwest Nepal. Journal of Ethnopharmacology, 163:210–9. PMID: 25655999. https://doi.org/
Mahmoud, T., Gairola, S., 2013. Traditional Knowledge and Use of Medicinal Plants in the Eastern Desert of Egypt: A Case Study from Wadi El-Gemal National Park. Journal of Medicinal Plants Studies, 1, 10-17. https://www.scirp.org/reference/referencespapers?referenceid=3143895
Mathibela, M.K., Egan, B.A., Du Plessis, H.J., Potgieter, M.H., 2015. Socio-cultural profile of Bapedi traditional healers as indigenous knowledge custodians and conservation partners in the Blouberg area, Limpopo Province, South Africa. Journal of Ethnobiology and Ethnomedicine, 11:49. DOI https://doi.org/
Mahwasane, S.T.L., Middleton, L.N., Boaduo, N., 2013. An ethnobotanical survey of indigenous knowledge on medicinal plants used by the traditional healers of the Lwamondo area, Limpopo province, South Africa. South African Journal of Botany, 88, 69–75. https://www.ethnopharmacologia.org/prelude2020/pdf/biblio-hm-55-mahwasane.pdf
Maramba-Lazarte, C. 2020. Benefits of Mainstreaming Herbal Medicine in the Philippine Healthcare System. Acta Medica Philippina, 54(1). https://doi.org/10.47895/amp.v54i1.1078
Menale, B., De Castro, O., Cascone, C., Muoio, R., 2016. Ethnobotanical investigation on medicinal plants in the Vesuvio National Park (Campania, Southern Italy). Journal of Ethnopharmacology. http://dx.doi.org/10.1016/j.jep.2016.07.049
Mendoza, L.A., Lagbas, A.J., Buot Jr., I.E., 2016. Conservation status of the plant species in selected areas with frequent human activities in Roosevelt Protected Landscape, Bataan, Luzon Island, Philippines. Thailand Nat His Mus J, 10(2), 79-115. https://www.researchgate.net/publication/312551606_Conservation_Status_of_the_Plant_Species_in_Selected_Areas_with_Frequent_Human_Activities_in_Roosevelt_Protected_Landscape_Bataan_Luzon_Island_Philippines
Meniza, J.F., Pasco, M.M., Alimbon, J.A., 2024. A review of ethnobotanical studies reveals over 500 medicinal plants in Mindanao, Philippines. Plant Diversity, 46, 551-564. https://pubmed.ncbi.nlm.nih.gov/39290882/
Mesfin, K., Tekle, G., Tesfay, T., 2013. Assessment of threatening factors of medicinal plants species in Samre District, South-eastern Tigray, Northern Ethiopia. Journal of Medicinal Plant Studies, 1, 38-42. ISSN 2320-3862. https://www.plantsjournal.com/vol1Issue1/Issue_july_2013/14.1.pdf
Miano, R.S., Picardal, J.P., Alonso, C.A., Reuyan, D., 2011. Ethnobotanical inventory and assessment of medically-important plant roots in Cebu Island, Philippines. Asian Journal of Biodiversity. CHED Accredited Research Journal, Category A, 2, 81-102. ISSN 2094-1519. https://www.researchgate.net/publication/314913900_Ethnobotanical_Inventory_and_Assessment_of_Medically-Important_Plant_Roots_in_Cebu_Island_Philippines
Motaleb, M.A., Firoz, R., Adrika, A., Khan, N.A., 2010. Approaches to conservation of medicinal plants and traditional knowledge: A focus on the Chittagong Hill Tracts. International Union for Conservation of Nature, Keidanren Nature Conservation Fund, Bangladesh Country Office, Dhaka, Bangladesh, pp viii+30. https://portals.iucn.org/library/sites/library/files/documents/2010-030.pdf
Okigbo, R.N., Eme, U.E., Ogbogu, S., 2008. Biodiversity and conservation of medicinal and aromatic plants in Africa. Biotechnology and Molecular Biology Reviews, 3(6), 127-134. ISSN 1538-2273. https://academicjournals.org/journal/BMBR/article-full-text-pdf/2EFEB8C40238
Oladele, A. T., Alade, G. O., Omobuwajo, O.R., 2011. Medicinal plants conservation and cultivation by traditional medicine practitioners (TMPs) in Aiyedaade Local Government Area of Osun State, Nigeria. Agriculture and Biology Journal of North America. ISSN 2151-7517. https://doi.org/
Ong, H.G., Kim, Y.D., 2014. Quantitative ethnobotanical study of the medicinal plants used by the Ati Negrito indigenous group in Guimaras Island, Philippines. Journal of Ethnopharmacology, 157, 228-242. https://doi.org/
Otieno, N. E., Analo, C., 2012. Local indigenous knowledge about some medicinal plants in and around Kakamega forest in western Kenya. F1000Research. https://doi.org/
Oyebode, O., Kandala, N.B., Chilton, P.J,, Lilford, R.J., 2016. Use of traditional medicine in middle-income countries: a WHO-SAGE study. Health Policy and Planning, 31, 984–99, doi: https://doi.org/
Paraguison, L.D.R., Tandang, D.N., Alejandro, G.J.D., 2020. Medicinal plants used by the Manobo tribe of Prosperidad, Agusan del Sur, Philippines: An ethnobotanical survey. Asian Journal of Biological and Life Sciences, 9, 326e333. https://doi.org/10.5530/ajbls.2020.9.49.
Posey, D.A., 1996. Protecting indigenous peoples’ rights to biodiversity. Environment: Science and Policy for Sustainable Development, 38(8), 6-45. DOI: https://doi.org/.
Semenya, S.S., Potgieter, M.J., 2014. Bapedi traditional healers in the Limpopo Province, South Africa: Their socio-cultural profile and traditional healing practice. Journal of Ethnobiology and Medicine, 10(4). https://ethnobiomed.biomedcentral.com/articles/10.1186/1746-4269-10-4
Soetan, K. O., Aiyelaagbe, O. O., 2009. The need for bioactivity-safety evaluation and conservation of medicinal plants – A review. Journal of Medicinal Plants Research, 3(5), 324-328. ISSN 1996-0875. https://www.researchgate.net/publication/242035192_The_need_for_bioactivity-safety_evaluation_and_conservation_of_medicinal_plants_-_A_review
Stofferson, A., Winstrup, M., Nieminen, R., Allerton, T., 2011. The sustainability of medicinal plant use in the local culture in Ongeluksnek, Eastern Cape, South Africa. Interdisciplinary Land Use and Natural Resource Management. Faculty of Life Sciences, University of Copenhagen. https://sluse.dk/project/South-Africa_medicinal_plants_and_traditional_healing_in_contemporary_rural_south_africa.pdf
Struthers, R., 2003. The Artistry and Ability of Traditional Women Healers, Health Care for Women International, 24:4, 340-354. https://pubmed.ncbi.nlm.nih.gov/12746005/
Tali, B.A., Ganie, A. H., Nawchoo, I. A., Wani, A. A., Reshi, Z. A., 2014. Assessment of threat status of selected endemic medicinal plants using IUCN regional guidelines: A case study from Kashmir Himalaya. Journal for Nature Conservation. https://doi.org/10.1016/j.jnc.2014.06.004
Teves, R.M., Tangtengco, O.A.G., Sumatra, R.U., Carag, H.M., Isidro-Lapena, J.S., 2023. Ethnomedicinal survey of valuable plants used by Eskaya traditional healers in Bohol Island, Philippines. Acta Med Philipp., 57(3), 17-27. https://doi.org/10.47895/amp.vi0.3883.
Vandebroek, T.E., Goetghebeur, P., Sanca, S., Arrazola, S., Van Damme, P., 2008. The relationship between plant use and plant diversity in the Bolivian Andes, with special reference to medicinal plant use. Human Ecology, 36(6):861–79. https://www.researchgate.net/publication/226977713_The_Relationship_Between_Plant_Use_and_Plant_Diversity_in_the_Bolivian_Andes_with_Special_Reference_to_Medicinal_Plant_Use
Wilcox, M.L., Bodeker, G., 2004. Traditional Herbal Medicines for Malaria. British Medical Journal, 329, 1156-1159. https://doi.org/10.1136/bmj.329.7475.1156
World Health Organization (WHO), International Union for Conservation of Nature and Natural Resources (IUCN), World Wide Fund for Nature (WWF), 1993. Guidelines on conservation of medicinal plants. ISBN 2-8317-0136-8. https://iris.who.int/bitstream/handle/10665/41651/2831701368_en.pdf